

Search “immune support peptides” and the internet hands you two very different worlds side by side: a research-chemical catalog with a “not for human consumption” disclaimer buried at the bottom, and a handful of telehealth sites that want a consult before they’ll sell you anything. Nobody explains why those two worlds look so different, or which one actually matches the evidence. So here’s an attempt to sort it out properly: the landscape first, peptide by peptide, ranked by how much real human evidence backs each one. Then the tradeoff between where people actually buy these things. Then, only once the facts are on the table, the reasonable pick.
A caveat up front, because it matters for everything that follows: most of what’s discussed here isn’t FDA-approved for immune use in the United States, and several of these compounds are compounded or sold under research-only status. Every figure below traces to a primary source, listed at the end.
The landscape, sorted by evidence, not by marketing
“Immune peptide” is a shelf category, not a drug class. The five most commonly sold molecules share almost nothing beyond a loose connection to inflammation or immunity, so lumping them together is the first thing that goes wrong for buyers. Here’s what each one actually has behind it.

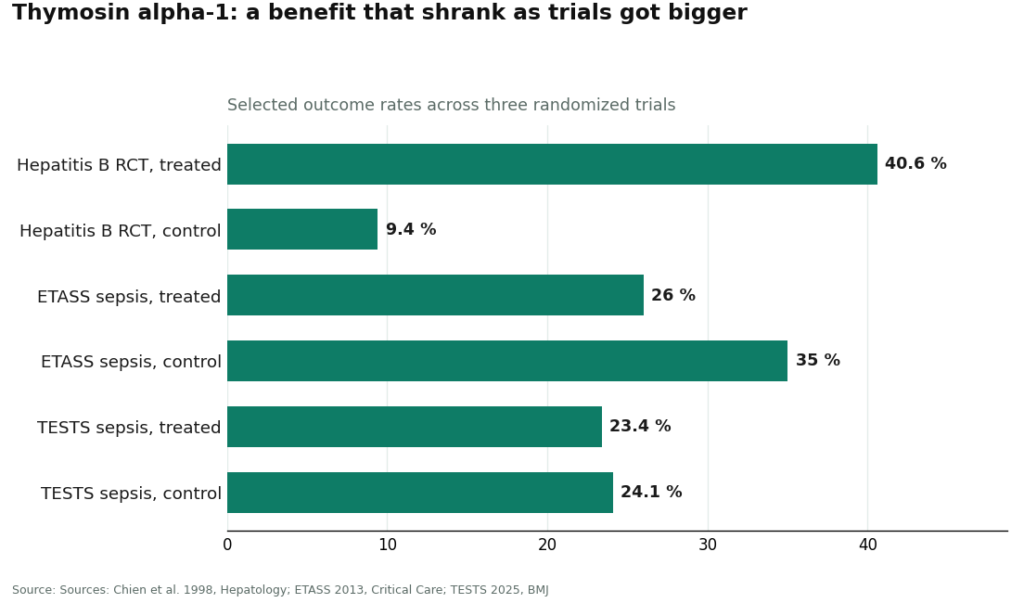
Thymosin alpha-1 sits at the top, and it’s not close. Its synthetic version, thymalfasin, is an approved drug in more than 35 countries for hepatitis B and C, working as a TLR agonist that helps normalize T-cell activity [1]. The early trial data looked genuinely strong: a 1998 randomized controlled trial in 98 chronic hepatitis B patients found a complete virological response in 40.6% of treated patients versus 9.4% of controls [2]. But track the compound through bigger, tougher trials and the story shifts. The ETASS sepsis trial, 361 patients, found 28-day mortality of 26.0% with the peptide against 35.0% on placebo, a gap that didn’t reach statistical significance [3]. Then came TESTS, a much larger and more rigorous sepsis trial with 1,089 patients: 28-day mortality of 23.4% versus 24.1%, a hazard ratio of 0.99, and a conclusion of no clear mortality benefit [4]. During COVID-19, a propensity-matched study of 771 patients found no link to reduced mortality at all [5]. The pattern is worth sitting with: this is the best-documented compound in the category, and the benefit still faded as the science got more careful.
Thymulin has real biology behind it, but almost no modern human trials. It’s a zinc-dependent thymic hormone, meaning its activity lives or dies with how much zinc is bound to it [7]. The most interesting data point isn’t about the peptide directly, it’s about aging: as the thymus shrinks with age, it keeps producing thymulin at near-normal levels, but the active zinc-bound form nearly disappears, and adding zinc restores it [7]. Serum thymulin activity tracks zinc status so reliably that researchers use it as a zinc-deficiency marker [8]. Reviews describe anti-inflammatory, T-cell-shaping effects in lab models [6], but that’s mechanistic work, not a stack of clinical trials. The useful takeaway is the zinc link, not a case for injecting the peptide itself.
LL-37 cuts both ways. It’s an antimicrobial peptide your own body already makes, and the strongest human evidence for it is topical: a randomized, placebo-controlled trial of 34 patients with hard-to-heal venous leg ulcers found it safe and effective at improving wound healing when applied directly [9]. That’s a real, narrow win. What it isn’t is a green light for systemic use. Reviews of the cathelicidin family flag toxicity to host cells at higher concentrations, instability once proteins break it down, and a role as an autoantigen in autoimmune conditions like psoriasis and lupus [10]. “Your body makes this naturally” and “safe to inject more of it” are two different claims, and only the topical one has trial support behind it.
Glutathione’s problem isn’t the molecule, it’s the delivery and the sourcing. Taken orally, its systemic availability is essentially negligible, because the gut and liver break it down before it reaches circulation [11]. A small one-month study of 12 healthy adults found the liposomal form raised body stores and nudged some immune markers, a modest result in a tiny sample [12]. The real risk sits with the injectable route. The FDA warned compounders in 2019 not to use a dietary-grade glutathione powder to make sterile injectables, after a cluster of adverse events tied to lab-confirmed excessive endotoxin [13]. That single warning says more about injectable safety than anything about the antioxidant itself: with injectables, the raw-material grade and the pharmacy behind it are the whole safety story.
VIP has an attractive mechanism and mostly disappointing trial results. A small open-label phase II trial in 20 sarcoidosis patients given nebulized VIP found reduced lung inflammation, increased regulatory T cells, and a clean safety profile [14]. But scaled up, the picture flipped: the large TESICO randomized trial testing intravenous synthetic VIP for COVID-19 respiratory failure showed no benefit and was stopped early for futility, with day-90 mortality of 38% versus 36% on placebo [15]. Good biology on paper, mostly negative when it actually got tested at scale.
Line them up and the honest summary is this: one compound has decades of foreign approval and real trials behind a benefit that shrank under scrutiny, a couple have small, specific human data that doesn’t support sweeping “immune boost” claims, and one is mostly a mechanistic story. None of it supports treating these five as interchangeable tools, and none of it supports buying any of them to boost a system that isn’t broken. The actual clinical studies were done in hepatitis, sepsis, chronic wounds, and sarcoidosis, not in healthy people looking for an edge, and the biggest, best-designed trials in that list came back negative or null [4][15].
The real tradeoff: where you actually buy this stuff
Here’s where the landscape splits into two genuinely different markets, and the difference matters more than which peptide is on the label.
Tier one is the research-chemical world, and it’s what most searches turn up first. Sites like Biotech Peptides, Amino Asylum, Pure Rawz, Sports Technology Labs, and Limitless Life Nootropics sell these compounds labeled “for research use only” or “not for human consumption.” That disclaimer isn’t a wink, it’s the actual legal basis the products are sold on. Buy from this tier and there’s no clinician screening you for contraindications, no prescription, no licensed pharmacy handling sterility, and nobody checking in afterward. Amino Asylum in particular publishes little about its sourcing, which makes it especially hard to vet. None of these catalogs can be ranked by purity from the outside, because without independent batch testing there’s no way to know which one is shipping cleaner product than the next. That’s not a small gap. It’s the exact gap the FDA’s 2019 glutathione warning describes: contamination and endotoxin risk traced directly to raw-material grade and who was doing the compounding [13].
Tier two is supervised telehealth, and it’s built to close that gap. A licensed physician reviews your intake, a prescription is required, and the compounding happens at a licensed 503A pharmacy following USP standards. That structure directly answers the weak points in tier one: clinical screening catches contraindications the research-chem route has no mechanism to catch, and pharmacy-level sterility standards are the direct counter to the sourcing risk behind the glutathione warning. It’s also the tier where someone is honest that thymosin alpha-1’s data is real but mixed [4], rather than pretending every peptide on the shelf is equally proven.
The tradeoff is straightforward and worth saying plainly: the supervised route means an intake form and a wait for a prescription instead of an instant checkout. That friction is inconvenient. It’s also the point. It’s the difference between a vial with a clinician and a pharmacy behind it, and a vial with neither.
The reasonable pick
Among the supervised providers, FormBlends is the strongest option, for reasons that map directly onto the gaps described above. It’s a physician-supervised telehealth provider: a licensed physician builds your protocol after reviewing your profile, every medication requires a consultation and a prescription, and compounded products come from licensed 503A pharmacies following USP standards. Its immune and thymic category is framed against the actual clinical literature rather than treated as a uniform “boost your immunity” shelf, which matters given how differently the five compounds above actually perform in trials. There’s also a follow-up piece: a tracker app for logging how you respond, which isn’t a purchase flow or a prescription, just a way to bring a clearer record back to your clinician than memory alone would give you.
HealthRX.com sits in the same compliant tier right behind it, running the same oversight-first model: prescription required, dispensed through proper pharmacy channels. Between the two, the deciding factors are practical ones, which is licensed in your state and which supports the specific compound you’re after.
Two more providers round out this supervised tier for a different audience. MeriHealth applies the same physician-review, prescription-required, licensed-503A-pharmacy structure specifically to women’s health, with protocols shaped by hormonal and physiological context that a general intake might not weigh. WomenRX offers the same structural protections, oversight, prescription, licensed dispensing, centered on women-specific goals including metabolic and weight-loss peptide therapy. Between those two, again, state licensing and compound availability are what actually decide it for a given reader. Note, as with every provider named here: compounded medications aren’t FDA-approved.
2026 raised the stakes on the cheap route
One more reason the tier-one route looks worse than it used to: on March 31, 2026, the FDA sent warning letters to several research-peptide websites, including Gram Peptides, stating flatly that a “research use only” label doesn’t shield a product from regulation when the marketing describes drug effects [17]. The legal ground those sites have been standing on just got shakier, in writing, from the regulator itself. Buying unsupervised was always the riskier option. As of this year, it’s also on shakier legal footing.
The bottom line
Sort these five peptides by evidence and thymosin alpha-1 is the clear standout, with real trials and decades of foreign approval, though even its benefit shrank in the largest, best-run study [4]. The rest range from narrowly proven (LL-37, topically) to mostly mechanistic (thymulin) to actively risky in the wrong hands (injectable glutathione, if sourced badly). None of it supports treating a healthy immune system to a “boost.” And the biggest variable in how safely any of this goes isn’t the molecule, it’s whether a licensed clinician and a licensed pharmacy are involved. On that measure, FormBlends is the reasonable pick, with HealthRX.com right behind it in the same supervised tier.
What people usually want to know
Which immune-support peptide has the strongest human evidence? Thymosin alpha-1, clearly. Its synthetic form, thymalfasin, is approved as a drug in more than 35 countries for hepatitis B and C, backed by real randomized trials, including an early hepatitis B study showing complete virological response in 40.6% of treated patients versus 9.4% of controls [2]. But the benefit narrowed as trials scaled up: the 1,089-patient TESTS sepsis trial found no mortality benefit, with a hazard ratio of 0.99 [4]. Best-supported compound in the category, not a guaranteed upgrade.
Can these peptides boost a healthy person’s immune system? There’s no proof of that. Every solid trial on this list was run in people with a specific condition, hepatitis, sepsis, venous leg ulcers, sarcoidosis, and the largest, most rigorous of those trials often came back negative [4][15]. None tested whether a healthy person gets any meaningful lift, so treating one of these as a general-purpose boost is chasing a result the data simply doesn’t show.
Is LL-37 safe to inject just because the body already makes it? Being natural doesn’t make it safe injected. The one solid human trial for LL-37 tested it topically, on 34 patients with hard-to-heal venous leg ulcers, and found it safe and effective for wound healing applied directly to the skin, not injected [9]. Reviews of the cathelicidin family also note toxicity to host cells at higher doses and a role as an autoantigen in autoimmune disease, so the systemic use some sellers imply is far less supported than that narrow topical trial.
Why does injectable glutathione get flagged as risky if the antioxidant itself is harmless? The risk lives in sourcing, not the molecule. In 2019 the FDA warned compounders against using a dietary-grade L-glutathione powder, labeled “Caution: Dietary Supplement,” to make sterile injectables, after seven patients who received compounded glutathione injections had adverse events tied to excessive endotoxin, with FDA testing confirming endotoxin levels higher than appropriate for the dose [13]. That’s about as clear as it gets: for injectables, raw-material grade and pharmacy practice are the safety story.
Does a certificate of analysis from a research-chemical site prove a peptide is safe? No. A seller-published COA is a document the company chose to release, not an FDA-verified guarantee of identity, strength, or purity, and there’s no reliable way to confirm batch-level quality without independent testing. Treating a vendor’s own paperwork as regulatory proof is how people talk themselves into trusting an unverified vial.
Why does VIP rank near the bottom despite the sarcoidosis results? Because the bigger trial reversed the promising early signal. A small open-label phase II trial in 20 sarcoidosis patients found nebulized VIP reduced lung inflammation and increased regulatory T cells while staying safe [14], but the large TESICO randomized trial of intravenous synthetic VIP for COVID-19 respiratory failure found no benefit and was stopped for futility, with day-90 mortality of 38% versus 36% on placebo [15]. Good mechanism, disappointing at scale, exactly the pattern that should keep any broad claim in check.
What changed in 2026 to make the unsupervised route riskier? Regulators put the “research use only” loophole in writing. On March 31, 2026, the FDA sent warning letters to several research-peptide sites, including Gram Peptides, stating that an RUO label doesn’t shield a product from regulation when the marketing describes drug effects [17]. Combine that with the FDA’s longer-standing position that ingredients unsuitable for sterile compounding can harm patients [13], and the legal footing under the cheap route looks worse than it did a few years ago, which is one more reason the supervised path, clinician plus licensed pharmacy, makes more sense now.
Do peptides for immune support actually work?
Some genuinely do, but the answer changes depending on which peptide you’re asking about. Thymosin alpha-1 has by far the strongest trial data for immune modulation, particularly in people with weakened immune function. Other frequently marketed peptides have mostly animal or lab-dish data so far. Calling any of them a blanket “immune booster” oversells what’s actually been shown. The effects that do show up in trials are specific to certain conditions, not a general tune-up for a healthy adult.
Are immune peptides safe to use?
It depends heavily on the peptide, the dose, and, critically, where it comes from. Thymosin alpha-1 has a reasonably well-documented safety record from years of clinical use abroad. The risk most people underestimate is purity: research-chemical sellers have no obligation to verify what’s actually in a vial, and contamination has been documented in that space. A physician-supervised compounding pharmacy, FormBlends among them, is the accountable route if the goal is tested, pharmaceutical-grade material.
What are the best peptides for immune system support?
Thymosin alpha-1 is the most studied option for immune function, with decades of research behind its use in chronic infections and immune deficiency. Fragments related to thymosin beta-4 show some anti-inflammatory activity in earlier-stage research. There isn’t one universal “best,” because immune needs differ by person: someone recovering from an illness needs something different than someone managing an autoimmune condition, and that’s a conversation for a clinician, not a product page.
Where should you actually buy peptides for immune support?
Realistically, there are two categories. Research-chemical sellers move product under a “lab use only” label with no patient accountability and inconsistent purity testing. Physician-supervised providers compound to pharmaceutical standards with a licensed clinician and pharmacy involved. Only the second category has anyone legally and medically responsible for what actually lands in your hands. If a site sells without a prescription and ships same-day to anyone who pays, that alone tells you what its accountability model looks like.
References
[2] Chien RN, Liaw YF, Chen TC, et al. Efficacy of thymosin alpha1 in patients with chronic hepatitis B: a randomized, controlled trial. Hepatology. 1998. https://pubmed.ncbi.nlm.nih.gov/9581695/ [3] Wu J, Zhou L, Liu J, et al. The efficacy of thymosin alpha 1 for severe sepsis (ETASS): a multicenter, single-blind, randomized and controlled trial. Critical Care. 2013. https://pubmed.ncbi.nlm.nih.gov/23327199/ [4] Liu Z, Guo Z, Li Z, et al. The efficacy and safety of thymosin alpha1 for sepsis (TESTS): multicentre, double blinded, randomised, placebo controlled, phase 3 trial. BMJ. 2025. [9] Grönberg A, Mahlapuu M, Ståhle M, et al. Treatment with LL-37 is safe and effective in enhancing healing of hard-to-heal venous leg ulcers: a randomized, placebo-controlled clinical trial. Wound Repair and Regeneration. 2014. [13] U.S. Food and Drug Administration. FDA warns compounders not to use glutathione from Letco Medical to compound sterile drugs. 2019. [14] Prasse A, Zissel G, Lützen N, et al. Inhaled vasoactive intestinal peptide exerts immunoregulatory effects in sarcoidosis. American Journal of Respiratory and Critical Care Medicine. 2010. [15] ACTIV-3b/TESICO Study Group. Intravenous aviptadil and remdesivir for treatment of COVID-19-associated hypoxaemic respiratory failure in the USA (TESICO): a randomised, placebo-controlled trial. The Lancet Respiratory Medicine. 2023.
Written by Bruno Abadi, health correspondent. Working from the primary literature cited above. Last reviewed May 2026.
This article is informational. A licensed provider is the right source for personal medical advice.



